Cost‑Effective Policies and the Role of CDT in Detecting Chronic Alcohol Use
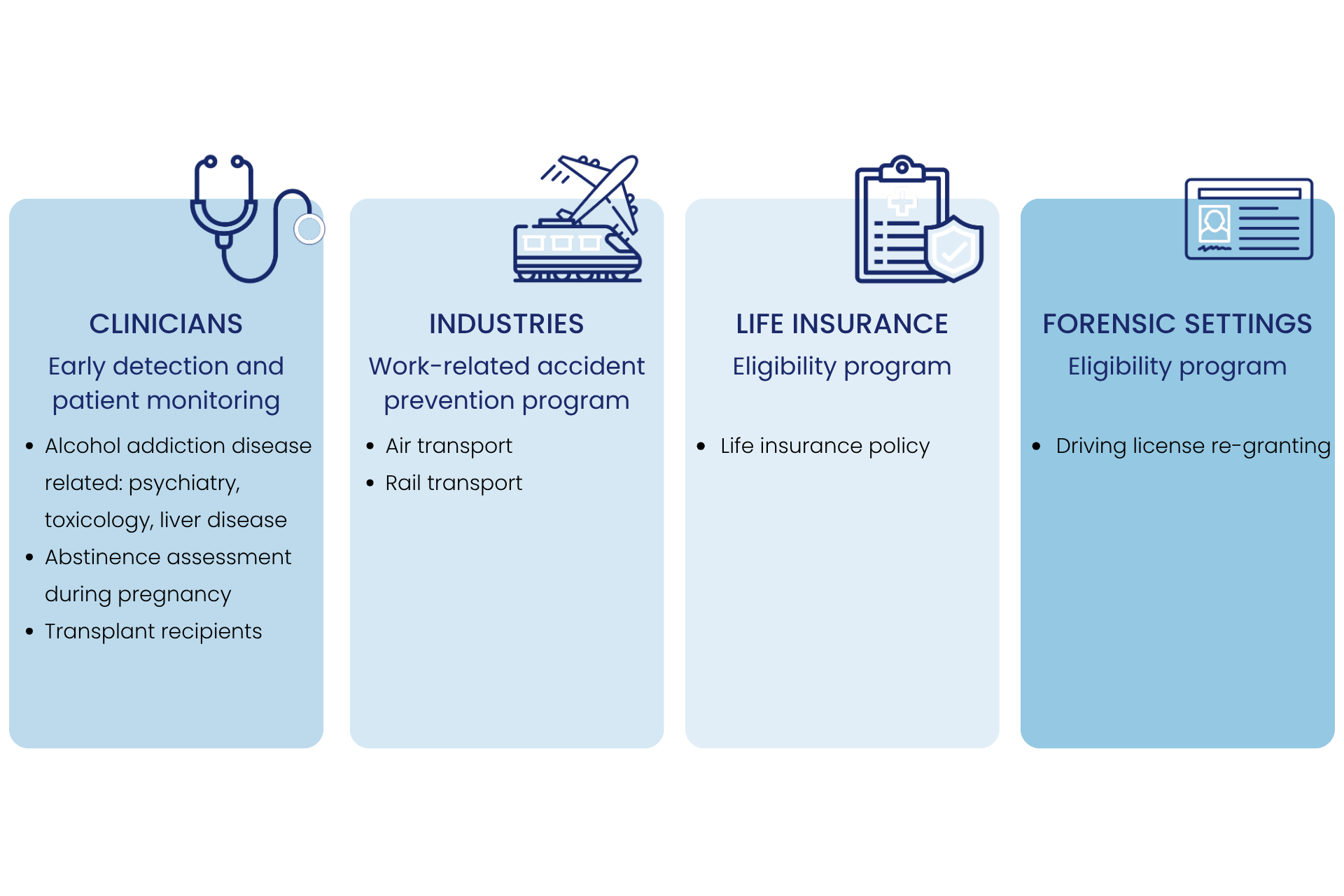
Implementing cost‑effective policies for the detection, diagnosis, and monitoring of alcohol misuse in clinical, industrial, and forensic settings can significantly improve clinical outcomes, reduce drink‑driving incidents, diminish workplace accidents, and ultimately lower the economic burden associated with alcohol‑related harm. Carbohydrate‑Deficient Transferrin (CDT) is recognized for its reliability as blood biomarker for chronic excessive alcohol consumption. Daily alcohol intake exceeding approximately 60 g per day over a period of about two weeks leads to an increase in CDT levels, reflecting alcohol‑induced disruption of normal liver cell function. In most individuals, elevated CDT values return to normal after several weeks of abstinence. CDT is highly specific for heavy drinking, and a 30% reduction in CDT indicates a meaningful decrease in alcohol intake. In many respects, CDT behaves similarly to HbA1c and other biochemical markers that vary according to lifestyle or therapeutic interventions. A rising CDT level serves as an objective indicator of relapse into heavy alcohol use, making it a sensitive and specific monitoring tool for healthcare professionals. CDT is the recommended marker for chronic alcohol use assessment by the IFCC.